
Talk Therapy for Bipolar Disorder: A Full Guide
Quick Answer: Talk therapy for bipolar disorder works alongside medication to reduce relapse rates by roughly 40%, improve daily functioning, and help you recognize mood shifts before they spiral. Family-focused therapy, interpersonal and social rhythm therapy, and cognitive-behavioral therapy each target different aspects—family stress, daily routines, or thought patterns—with sessions typically running 12-20 weeks and showing the strongest results when you’re stable rather than in crisis.
Last updated: May 8, 2026
Key Takeaways
- Talk therapy cuts relapse risk significantly when combined with medication, with some approaches reducing your odds of another episode by more than half over 1-4 years
- Different therapies target different triggers: family-focused therapy addresses relationship stress, IPSRT stabilizes your sleep and daily rhythms, CBT reshapes negative thought loops
- Timing matters more than you’d think—therapy works best during stable periods or right after an episode, not during acute mania
- Family involvement amplifies results, especially if your household runs high on conflict or criticism
- Depression responds better than mania across most talk therapies, though group psychoeducation shows promise for manic symptoms
- Effects can fade without maintenance—many people benefit from occasional booster sessions after the initial 12-20 weeks
- Dropout rates hover around 10-20%, lower than medication-only approaches, suggesting therapy feels more tolerable to most people
What Is Talk Therapy for Bipolar Disorder and How Does It Work?
Talk therapy for bipolar disorder is structured psychotherapy delivered alongside your medication to address the psychological, social, and behavioral dimensions that pills alone can’t fix. You meet with a trained therapist—individually, with family, or in groups—to learn skills that prevent relapses, stabilize routines, improve relationships, and catch early warning signs of mood shifts.
The core types include:
- Cognitive-Behavioral Therapy (CBT): Challenges distorted thinking patterns that fuel depression or risky behavior
- Interpersonal and Social Rhythm Therapy (IPSRT): Regulates your daily schedule—sleep, meals, social time—to keep your internal clock steady
- Family-Focused Therapy (FFT): Teaches your household better communication and problem-solving to reduce conflict
- Dialectical Behavior Therapy (DBT): Builds emotional regulation skills, originally for borderline personality but adapted for bipolar’s intensity
- Group Psychoeducation: Educates you and peers about bipolar, medication adherence, and relapse triggers in a supportive setting
These therapies work by targeting mechanisms medication misses. Mood stabilizers calm your brain chemistry, but they don’t teach you how to handle a fight with your partner, fix a chaotic sleep schedule, or recognize the subtle irritability that precedes mania. Therapy fills those gaps. Research shows that when you combine talk therapy with pharmacotherapy, you stay well longer, function better at work and home, and feel more in control of your life.
Choose talk therapy if: You’ve had multiple relapses despite taking medication, your family relationships are strained, your daily routine is all over the place, or you struggle to stick with treatment. It’s especially useful after you’ve stabilized from an acute episode and want to prevent the next one.
For more context on how psychotherapy fits into your overall treatment plan, see our guide on does psychotherapy help to treat bipolar disorder.

How Does Family-Focused Therapy Prevent Relapses?
Family-focused therapy prevents relapses by lowering the emotional temperature in your household and teaching everyone—you and your loved ones—how to communicate without escalating conflict. FFT typically runs 12 sessions over four months, covering psychoeducation about bipolar, communication skills, and collaborative problem-solving.
Why it works: High expressed emotion (EE)—criticism, hostility, or over-involvement from family—predicts faster relapse. FFT directly targets this. Studies show people in FFT delay their next mood episode significantly longer than those getting brief education alone, with hazard ratios around 0.55 over 1-4 years. That means your risk of relapse drops by nearly half.
What happens in sessions:
- Psychoeducation phase: Your therapist explains bipolar’s biology, symptoms, and triggers to your family, reducing blame and misunderstanding
- Communication training: You practice active listening, expressing feelings without attacking, and asking for what you need clearly
- Problem-solving: The family identifies stressors—like chore conflicts or medication reminders—and works out solutions together
FFT works best if:
- Your family is involved and willing to attend sessions
- There’s noticeable tension, criticism, or conflict at home
- You’re in a stable or early recovery phase, not mid-crisis
Common mistake: Waiting until a crisis to start FFT. It’s preventive, not a firefighting tool. Begin when you’re stable so the skills are in place before stress hits.
One young woman I know started FFT after her third hospitalization. Her parents had been hovering, checking her pill bottles daily, which she experienced as suffocating. Through FFT, they learned to step back while she learned to update them proactively. Her next episode didn’t come for over two years—her longest stretch yet.
FFT also reduces suicidal thinking and helps adolescents at high risk for bipolar delay their first full episode. If you have kids showing early mood symptoms, FFT can be a game-changer. Learn more about family support strategies.
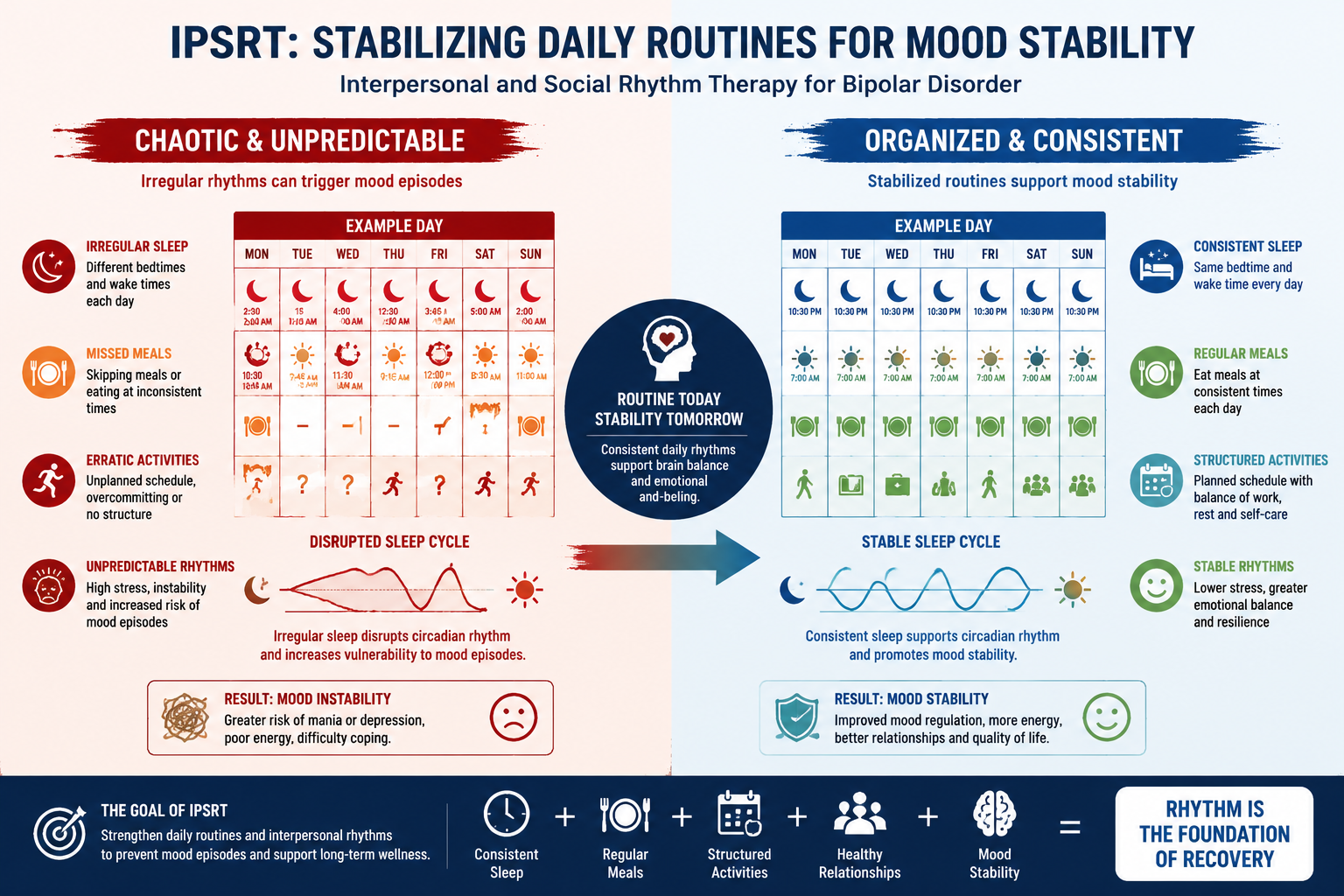
Can Interpersonal and Social Rhythm Therapy Stabilize Your Mood?
Interpersonal and social rhythm therapy stabilizes your mood by locking in consistent daily rhythms—wake time, meals, exercise, social contact—which in turn regulate your circadian biology. Bipolar disorder disrupts your internal clock, and chaotic schedules can trigger episodes. IPSRT treats the schedule itself as medicine.
How IPSRT works:
- Social Rhythm Metric (SRM): You track five daily activities (wake time, first contact with another person, start of work/school, dinner, bedtime) to identify irregularities
- Interpersonal focus: The therapist helps you resolve relationship conflicts or role transitions (job loss, breakup) that destabilize your routine
- Rhythm stabilization: You gradually shift toward consistent times, even on weekends, to keep your circadian system steady
Evidence: IPSRT improves overall functioning with effect sizes around -0.344 (small but meaningful) and reduces depressive symptoms more reliably than manic ones. In one trial, people receiving IPSRT had better social adjustment and fewer depressive episodes over 18 months compared to standard care, though relapse rates didn’t differ significantly—suggesting it’s more about quality of life than preventing all episodes.
IPSRT is ideal for:
- Shift workers or people with erratic schedules
- Those whose episodes follow sleep disruptions (like staying up all night before mania kicks in)
- Post-acute depression, where you’re rebuilding stability
Edge case: If you’re in acute mania, IPSRT won’t calm you down fast. It’s a maintenance tool, not an emergency brake.
I once worked with a freelance designer whose sleep schedule swung wildly—2 a.m. bedtimes one week, 10 p.m. the next. Her mood followed. IPSRT helped her set a non-negotiable 11 p.m. wind-down and 7 a.m. wake time, even if she had no morning meetings. Within three months, her depressive dips softened noticeably. She still had mood shifts, but they were gentler, less disruptive.
For more on managing daily rhythms, explore our resource on interpersonal and social rhythm therapy.
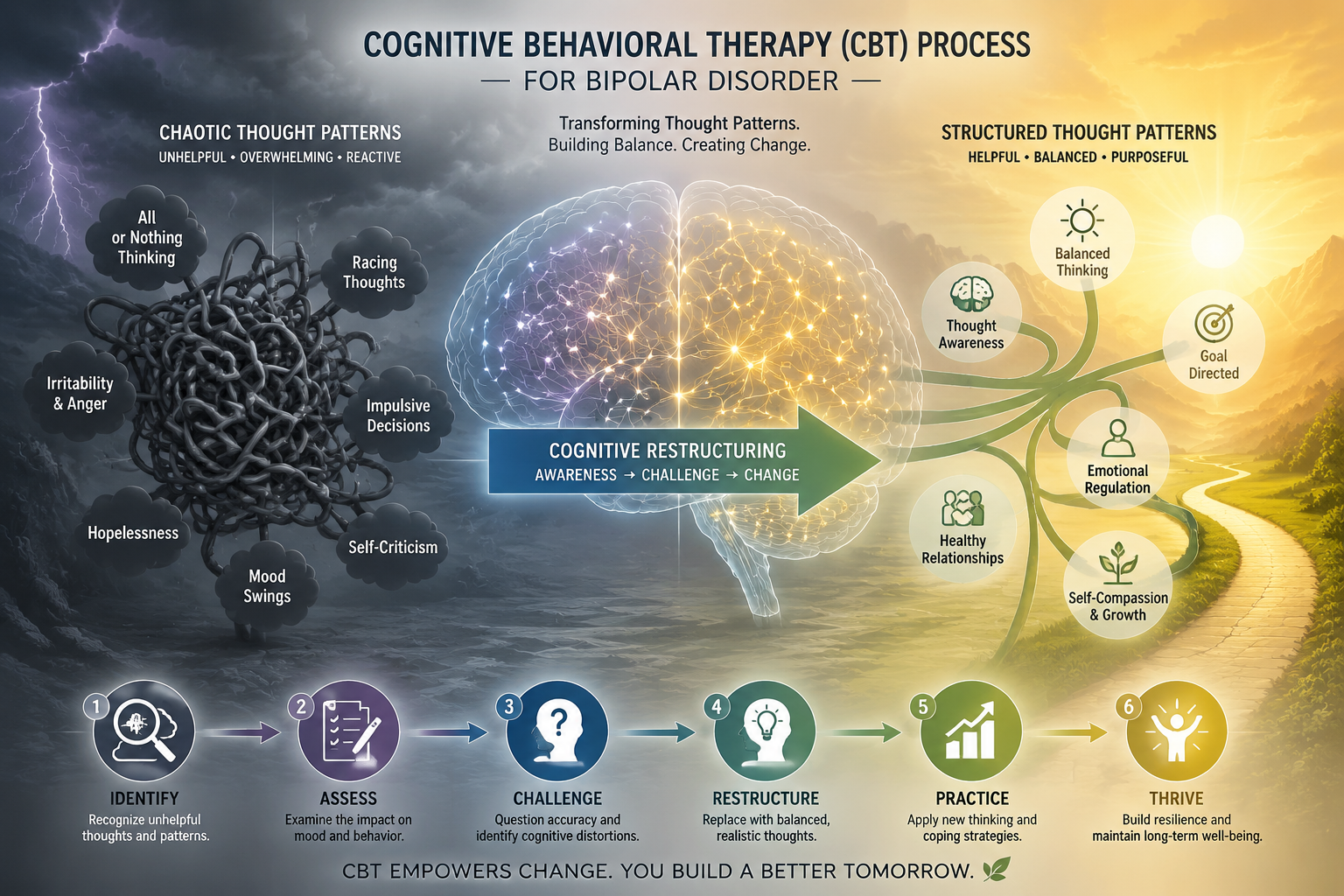
Does Cognitive-Behavioral Therapy Help With Bipolar Depression?
Cognitive-behavioral therapy helps with bipolar depression more than mania, offering modest but real symptom relief when added to medication. CBT teaches you to identify and challenge the negative, distorted thoughts that deepen depression—like “I’ll never get better” or “I’m a burden”—and replace them with balanced, evidence-based alternatives.
What CBT involves:
- Cognitive restructuring: Spotting automatic negative thoughts and testing their accuracy
- Behavioral activation: Scheduling activities that boost mood, even when you don’t feel like it
- Relapse prevention: Learning your personal warning signs (irritability, racing thoughts, sleep changes) and creating action plans
The evidence: Meta-analyses show CBT reduces depressive symptoms with effect sizes around -0.29 compared to treatment as usual—small, but enough to notice in daily life. Over two years, people in CBT spend fewer days in depressive episodes and function better socially. However, CBT doesn’t significantly reduce mania or long-term relapse rates in the final 18 months without booster sessions.
CBT works best for:
- Depressive-dominant bipolar (more time depressed than manic)
- People who can engage in homework between sessions
- Stable or post-acute phases, not during severe depression or mania
Common mistake: Expecting CBT to prevent mania. It’s not designed for that. If you’re prone to manic episodes, pair CBT with therapies like psychoeducation or FFT that address mania triggers.
Cost-effectiveness: One 30-month study found CBT reduced healthcare use and costs compared to usual care, making it a smart investment for both you and the system.
A friend with bipolar II used CBT to tackle the hopelessness that crept in every winter. Her therapist had her track evidence for and against thoughts like “Nothing I do matters.” Over 16 weeks, she built a mental toolkit—journaling, scheduling one social event weekly, challenging catastrophic predictions. Her depressive episodes still came, but they were shorter and less paralyzing.
For a broader look at treatment options, check out bipolar disorder treatment.
What Are the Benefits of Group Psychoeducation and Support?
Group psychoeducation and support reduce relapse and boost adherence by teaching you and others with bipolar about the disorder, medications, and early warning signs in a shared, validating environment. You’re not just learning facts—you’re hearing how others manage the same struggles, which normalizes your experience and builds accountability.
Key benefits:
- Relapse prevention: Group psychoeducation cuts relapse odds by more than half (OR = 0.43) post-intervention, especially for manic symptoms
- Medication adherence: Hearing peers discuss side effects and benefits makes sticking with treatment feel less isolating
- Peer support: You gain practical tips (like how to handle a medication change or talk to your boss) that textbooks don’t cover
- Cost-effective: One therapist can help 8-12 people at once, making it accessible in community settings
What happens in group sessions:
- Education on bipolar biology, triggers, and treatment
- Sharing personal experiences and coping strategies
- Practicing communication or problem-solving skills together
- Monitoring mood and identifying early warning signs as a group
Group therapy is ideal if:
- You feel isolated or misunderstood
- You want to learn from others’ successes and mistakes
- Individual therapy feels too expensive or isn’t available
- You’re stable enough to engage without dominating or disrupting the group
Edge case: If you’re in acute mania or severe depression, group settings can be overwhelming or unproductive. Wait until you’re more stable.
One man I know joined a bipolar support group after his second hospitalization. He’d felt like the only person in the world who couldn’t “just stay on meds.” Hearing others describe the same struggle—the side effects, the denial, the fear of losing creativity—shifted something. He started attending regularly, and his adherence improved. He relapsed once more in three years, compared to three times in the prior three.
For more on peer support, see our article on the power of bipolar support groups.
How Do You Choose the Right Talk Therapy for Your Situation?
You choose the right talk therapy for bipolar by matching the therapy’s focus to your biggest challenges—family conflict, chaotic routines, depressive thinking, or emotional intensity—and considering your current mood phase and resources.
Decision framework:
| Your Main Challenge | Best Therapy | Why |
|---|---|---|
| High family tension or criticism | Family-Focused Therapy (FFT) | Directly reduces expressed emotion and teaches communication |
| Irregular sleep, meals, or schedule | Interpersonal and Social Rhythm Therapy (IPSRT) | Stabilizes circadian rhythms and daily routines |
| Persistent negative thoughts, hopelessness | Cognitive-Behavioral Therapy (CBT) | Challenges depressive thinking patterns |
| Intense emotions, impulsivity | Dialectical Behavior Therapy (DBT) | Builds emotional regulation and distress tolerance |
| Need for education and peer support | Group Psychoeducation | Cost-effective, normalizes experience, boosts adherence |
Phase considerations:
- Stable/maintenance phase: Any therapy works; this is the ideal time to start
- Post-acute depression: IPSRT or CBT to rebuild functioning and prevent relapse
- Post-acute mania: FFT or psychoeducation to address family stress and adherence
- Acute mania or severe depression: Therapy is less effective; focus on medication and crisis stabilization first
Practical factors:
- Family availability: FFT requires willing family members
- Schedule flexibility: IPSRT demands consistent session times and homework
- Cost: Group therapy is cheaper; check if your insurance covers individual sessions
- Therapist expertise: Not all therapists are trained in bipolar-specific approaches—ask about their experience
Common mistake: Starting therapy during a crisis and expecting immediate results. Therapy is preventive and skill-building, not a quick fix. If you’re in acute mania, stabilize with medication first, then begin therapy.
Pro tip: You can combine therapies. For example, start with CBT for depression, then add IPSRT to stabilize your routine, or do individual CBT alongside a family session every few weeks.
If you’re unsure, talk to your psychiatrist or a therapist trained in bipolar disorder. They can assess your situation and recommend the best fit. For more on working with your treatment team, see working with your doctor.
What Should You Expect During Talk Therapy Sessions?
During talk therapy sessions for bipolar, you’ll typically meet weekly for 45-60 minutes over 12-20 weeks, working through structured exercises, homework, and discussions tailored to your therapy type—whether that’s tracking your daily rhythms, practicing communication with family, or challenging negative thoughts.
General session structure:
- Check-in: Review your mood, sleep, medication adherence, and any significant events since last session
- Agenda setting: Decide what to focus on today (e.g., a conflict, a mood shift, a skill to practice)
- Core work: Engage in the therapy’s main techniques—cognitive restructuring, rhythm tracking, family role-plays, etc.
- Homework assignment: Practice skills between sessions (e.g., fill out a thought record, maintain a sleep schedule, have a planned conversation)
- Wrap-up: Summarize key points and plan for next week
Therapy-specific examples:
- CBT: You might bring a thought record where you logged a depressive thought (“I’m useless”), the situation that triggered it, and evidence for/against it. The therapist helps you generate a balanced alternative (“I’m struggling right now, but I’ve succeeded before”).
- IPSRT: You review your Social Rhythm Metric, noting that you stayed up until 2 a.m. twice this week. You and the therapist explore what disrupted your routine (stress at work?) and problem-solve how to protect your bedtime.
- FFT: Your family joins for a session. The therapist guides a role-play where you practice asking your partner for space without sounding angry, and your partner practices responding without defensiveness.
What to expect emotionally:
- Early sessions: You might feel hopeful, skeptical, or overwhelmed as you learn new concepts
- Middle sessions: Frustration is common when skills don’t work immediately or homework feels tedious
- Later sessions: Confidence grows as you see small wins—fewer arguments, better sleep, catching a mood shift early
Homework is non-negotiable. Therapy isn’t just the hour in the office; it’s practicing skills in real life. If you skip homework, progress stalls.
Dropout risk: About 10-20% of people drop out, often because sessions feel burdensome or they don’t see quick results. If you’re tempted to quit, talk to your therapist first. Sometimes adjusting the pace or focus makes a difference.
One woman I know hated the homework at first—tracking her sleep felt like one more chore. But after three weeks, she noticed a pattern: her mood dipped every time she slept less than six hours. That insight motivated her to protect her sleep, and her depressive episodes became less frequent. The homework paid off.
For more on what to expect in treatment, see dealing with bipolar disorder.
How Long Does Talk Therapy Take to Show Results?
Talk therapy for bipolar typically shows initial results within 8-12 weeks, with full benefits emerging over 6-12 months and sustained effects requiring occasional booster sessions beyond the initial treatment phase. The timeline varies by therapy type, your baseline stability, and how consistently you practice skills.
Phase-by-phase timeline:
- Weeks 1-4: You’re learning concepts, building rapport with your therapist, and starting to track patterns (thoughts, rhythms, family interactions). Mood changes are minimal, but awareness increases.
- Weeks 5-12: Skills start clicking. You catch a negative thought before it spirals, adjust your sleep schedule and feel steadier, or navigate a family conflict without blowing up. Small wins accumulate.
- Months 3-6: Functioning improves noticeably—fewer missed workdays, better relationships, more confidence. Relapse risk begins to drop.
- Months 6-12: Benefits plateau. You’ve internalized skills and your relapse rate is lower than before therapy. Some therapies (like CBT) show effects fading after 18 months without boosters.
- Beyond 1 year: Maintenance matters. Booster sessions every few months help sustain gains, especially for IPSRT and CBT.
Therapy-specific timelines:
- FFT: Relapse prevention effects appear within 6-12 months and strengthen over 1-4 years
- IPSRT: Functioning improvements emerge around 3-6 months; rhythm stabilization happens faster (weeks) but requires ongoing practice
- CBT: Depressive symptom relief shows within 8-16 weeks; relapse prevention is strongest in the first year
Factors that speed results:
- Starting therapy when stable, not in crisis
- Completing homework consistently
- High family involvement (for FFT)
- Fewer prior episodes (less than 12)
Factors that slow results:
- Comorbid substance use or PTSD
- Severe, frequent episodes (more than 12 lifetime)
- Inconsistent medication adherence
- Skipping sessions or homework
Common mistake: Expecting instant relief. Therapy is skill-building, not a light switch. If you’re not seeing progress by 12 weeks, talk to your therapist—maybe the approach needs tweaking, or maybe you need to address medication issues first.
One man I know started CBT after a depressive episode. He felt discouraged at week 6 because his mood hadn’t lifted. His therapist reminded him that CBT targets thinking patterns, which then influence mood over time. By week 10, he noticed he was catastrophizing less, and by week 14, his mood had improved. Patience paid off.
For more on managing symptoms over time, see bipolar disorder symptoms.
What Are the Limitations and Challenges of Talk Therapy?
Talk therapy for bipolar has real limitations: it’s less effective during acute mania, benefits can fade without maintenance, it requires time and effort that not everyone can sustain, and access to trained therapists is uneven, especially in rural or low-income areas.
Key limitations:
- Acute mania: Therapy doesn’t calm mania quickly. If you’re in a full manic episode, medication and crisis stabilization come first. Therapy works best after you’ve stabilized.
- Fading effects: CBT and IPSRT benefits often wane after 18-24 months without booster sessions. You can’t just “graduate” and forget the skills.
- Homework burden: Therapy demands practice between sessions—tracking moods, challenging thoughts, maintaining routines. If you’re overwhelmed or disorganized, this can feel impossible.
- Therapist availability: Not all therapists are trained in bipolar-specific approaches like FFT or IPSRT. Finding one can take time, and insurance may not cover enough sessions.
- Dropout rates: About 10-20% of people quit early, often because progress feels slow or sessions conflict with work/family demands.
Challenges by therapy type:
- FFT: Requires willing, available family members. If your family is abusive or unwilling, FFT won’t work.
- IPSRT: Demands rigid schedule adherence, which is hard if you work shifts, have young kids, or travel frequently.
- CBT: Focuses on depression; if mania is your main problem, CBT alone won’t cut it.
- Group therapy: Timing and group dynamics matter. If the group is dominated by one person or meets at inconvenient times, you may drop out.
Real-world barriers:
- Cost: Even with insurance, copays add up over 12-20 sessions. Without insurance, therapy can cost $100-$200+ per session.
- Stigma: Some people avoid therapy because they fear being judged or don’t believe it will help.
- Comorbidities: Substance use, PTSD, or ADHD complicate treatment and may require specialized approaches.
What to do about limitations:
- For fading effects: Schedule booster sessions every 2-3 months after finishing the main course of therapy.
- For homework burden: Start small—track just one thing (sleep time) instead of five. Build gradually.
- For access issues: Ask your psychiatrist for referrals, try teletherapy, or look for community mental health centers that offer sliding-scale fees.
- For acute mania: Don’t force therapy during crisis. Stabilize first, then start therapy to prevent the next episode.
Edge case: If you’ve had more than 12 prior episodes, therapy’s effects are smaller. You may need combined approaches—multiple therapies, longer treatment, or more intensive support.
One woman I know struggled with IPSRT because her job required frequent travel. Her therapist adapted by focusing on “anchor points”—non-negotiable sleep and meal times she could maintain even on the road. It wasn’t perfect, but it was better than giving up entirely.
For more on managing treatment challenges, see importance of staying on treatment.
How Does Talk Therapy Fit With Medication and Other Treatments?
Talk therapy fits with medication as a complementary partner, not a replacement—medication stabilizes your brain chemistry while therapy addresses the psychological, social, and behavioral factors that medication can’t touch, creating a more complete, durable recovery.
Why combine them:
- Medication alone often leaves residual symptoms—mild depression, relationship strain, poor sleep—that therapy can resolve.
- Therapy alone rarely prevents relapse in bipolar disorder, which has strong biological roots requiring pharmacological management.
- Together, they reduce relapse rates by roughly 40% more than medication alone, improve functioning, and boost adherence to both treatments.
How they work together:
- Medication (mood stabilizers, antipsychotics, antidepressants) regulates neurotransmitters, preventing extreme mood swings.
- Therapy teaches you to recognize early warning signs, manage stress, stabilize routines, and communicate better—skills that reduce triggers for episodes.
- Example: Lithium keeps your mood from spiking into mania, while IPSRT ensures you don’t stay up all night (a common mania trigger). Together, they’re more powerful than either alone.
Integrating with other treatments:
- Peer support groups: Complement therapy by providing ongoing community and practical tips. Therapy is structured skill-building; support groups are informal, long-term connection.
- Lifestyle changes: Therapy often incorporates sleep hygiene, exercise, and stress management, which reinforce medication’s effects. For more, see lifestyle changes.
- Wellness plans: Many therapists help you create a written plan for managing episodes, which you can share with your psychiatrist and family.
Medication adherence boost:
One of therapy’s biggest benefits is improving adherence. When you understand why you’re taking medication (psychoeducation), track how it helps (CBT), and have family support (FFT), you’re less likely to quit. Studies show therapy reduces non-adherence significantly.
Coordination matters:
Your therapist and psychiatrist should communicate, especially if you’re adjusting meds or experiencing side effects. If they don’t talk, you’re the bridge—update each on what the other is doing.
Common mistake: Stopping medication once therapy helps you feel better. Bipolar is chronic; you need both long-term. Therapy doesn’t cure the disorder—it helps you manage it alongside medication.
One man I know felt so good after 12 weeks of CBT that he tapered off his mood stabilizer without telling his doctor. Within two months, he was manic. He learned the hard way that therapy and medication are a team, not competitors.
For more on medication options, see bipolar disorder medications.
Frequently Asked Questions About Talk Therapy for Bipolar
How much does talk therapy for bipolar cost?
Therapy costs $100-$250 per session without insurance, with 12-20 sessions typical for initial treatment. Many insurance plans cover mental health therapy with copays of $20-$50 per session. Community mental health centers and sliding-scale clinics offer lower rates based on income. Teletherapy can be more affordable and accessible.
Can talk therapy replace medication for bipolar disorder?
No. Therapy alone rarely prevents relapse in bipolar disorder, which has strong biological components requiring medication. Therapy works best as an adjunct to mood stabilizers or other medications, addressing psychological and social factors that pills can’t fix. Stopping medication to rely only on therapy significantly increases relapse risk.
Which talk therapy is best for bipolar disorder?
It depends on your main challenges. Family-focused therapy (FFT) is best for family conflict, interpersonal and social rhythm therapy (IPSRT) for chaotic routines, cognitive-behavioral therapy (CBT) for depressive thinking, and dialectical behavior therapy (DBT) for emotional intensity. Group psychoeducation is cost-effective for education and peer support. Your therapist can help you choose.
Does talk therapy work during a manic episode?
Not effectively. Therapy is most useful during stable or post-acute phases, not during acute mania when your judgment and focus are impaired. If you’re manic, prioritize medication and crisis stabilization first, then start therapy once you’ve stabilized to prevent future episodes.
How long does talk therapy for bipolar last?
Initial treatment typically runs 12-20 weekly sessions (3-5 months), with benefits emerging around 8-12 weeks. Many people need booster sessions every 2-3 months after finishing to sustain gains, as effects can fade after 18-24 months without maintenance. Long-term, occasional therapy helps prevent relapse.
Can I do talk therapy online or does it have to be in person?
Teletherapy works well for bipolar disorder, offering the same benefits as in-person sessions with added convenience and access, especially in rural areas. Video sessions allow for real-time interaction, homework review, and skill practice. Some therapies (like FFT) may require occasional in-person family sessions, but most adapt easily to online formats.
What if my family won’t participate in family-focused therapy?
If your family is unwilling or unavailable, consider individual therapies like CBT or IPSRT that don’t require family involvement. You can also work with your therapist on communication skills to use with family on your own, or invite one supportive family member or friend to occasional sessions instead of the whole household.
Does insurance cover talk therapy for bipolar disorder?
Most insurance plans cover mental health therapy, including bipolar-specific approaches, though coverage varies. Check your plan’s mental health benefits, copays, and session limits. Many plans require a referral from your psychiatrist. If coverage is limited, ask about out-of-network benefits or sliding-scale community clinics.
Can talk therapy prevent bipolar episodes completely?
No therapy prevents all episodes, but it significantly reduces relapse risk—by roughly 40% in many studies—and makes episodes less severe and shorter when they do occur. Therapy is about management and resilience, not cure. Combined with medication, it offers the best chance of long-term stability.
What should I do if therapy isn’t helping after several weeks?
Talk to your therapist first. Progress can be slow, and adjustments to the approach or pace may help. If you’re not seeing any improvement by 12 weeks, consider whether you’re doing homework consistently, if medication needs adjustment, or if a different therapy type might fit better. Sometimes switching therapists or approaches is necessary.
Is group therapy as effective as individual therapy for bipolar?
Group psychoeducation is highly effective for relapse prevention and adherence, with some studies showing similar or better outcomes than individual therapy, especially for manic symptoms. However, individual therapy allows more personalized focus on your specific challenges. Many people benefit from both—individual sessions for deep work and group for peer support.
Can talk therapy help with bipolar depression specifically?
Yes. CBT and IPSRT both show moderate effectiveness for bipolar depression, reducing symptoms and improving functioning. CBT targets negative thought patterns, while IPSRT stabilizes routines that prevent depressive dips. However, therapy for bipolar depression is less effective than for unipolar depression, so medication remains essential.
Final Thoughts
Talk therapy for bipolar disorder isn’t a magic cure, but it’s a powerful tool that fills the gaps medication leaves behind. When you combine structured psychotherapy—whether family-focused, rhythm-based, or cognitive—with your mood stabilizers, you cut your relapse risk significantly, function better day-to-day, and gain skills to catch mood shifts before they derail your life.
The evidence is clear: therapy works, especially when you start during stable periods, stick with homework, and involve your family when possible.
Your next steps:
- Talk to your psychiatrist or therapist about which therapy fits your situation—family conflict, chaotic routines, or depressive thinking.
- Find a trained therapist experienced in bipolar-specific approaches. Ask about their training in FFT, IPSRT, or CBT for bipolar.
- Commit to the process—12-20 weeks of weekly sessions plus homework. Progress takes time, but small wins add up.
- Plan for maintenance—schedule booster sessions every few months after finishing to keep skills sharp and prevent relapse.
- Stay on your medication—therapy enhances medication, it doesn’t replace it. Both are essential for long-term stability.
You’re not alone in this.
Millions of people with bipolar disorder have walked this path, learned these skills, and built lives that work. Therapy is one more piece of the puzzle, and it’s worth the effort. Start today, and give yourself the best chance at a stable, fulfilling future.
For more resources and support, explore our bipolar disorder support page and connect with others who understand what you’re facing.