
Bipolar Disorder Medications
Quick Answer: Bipolar disorder medications work by stabilizing mood swings through three main classes: mood stabilizers like lithium prevent relapses and extend symptom-free periods to 81 months, atypical antipsychotics such as quetiapine treat both manic and depressive episodes with significant symptom reduction, and adjunctive antidepressants provide 40-60% response rates in depression when combined with stabilizers. Treatment success depends on matching medication type to your specific bipolar subtype, episode pattern, and individual response, with most people requiring long-term maintenance therapy to prevent recurrence.
Last updated: May 8, 2026
Key Takeaways
✅ Lithium remains the gold standard for bipolar I maintenance, preventing relapses for 81 months on average compared to 36 months with valproate
✅ Atypical antipsychotics work fast for both mania and depression, with quetiapine showing significant improvement within the first week
✅ Combination therapy often works best for refractory cases, with 33-100% of previously non-responsive patients showing improvement
✅ Antidepressants require caution in bipolar disorder, carrying up to 25% risk of triggering mania when used alone
✅ New medications arrived in 2026, including Bysanti for acute mania and novel lithium delivery systems entering trials
✅ Side effects vary widely by medication class, from lithium’s kidney concerns to antipsychotic weight gain
✅ Bipolar II responds differently than bipolar I, often benefiting more from lamotrigine and adjunctive antidepressants
✅ Regular monitoring is essential for safety, especially with lithium requiring blood level checks every 3-6 months
✅ Personalization matters more than protocols, as individual response varies significantly even within the same diagnosis
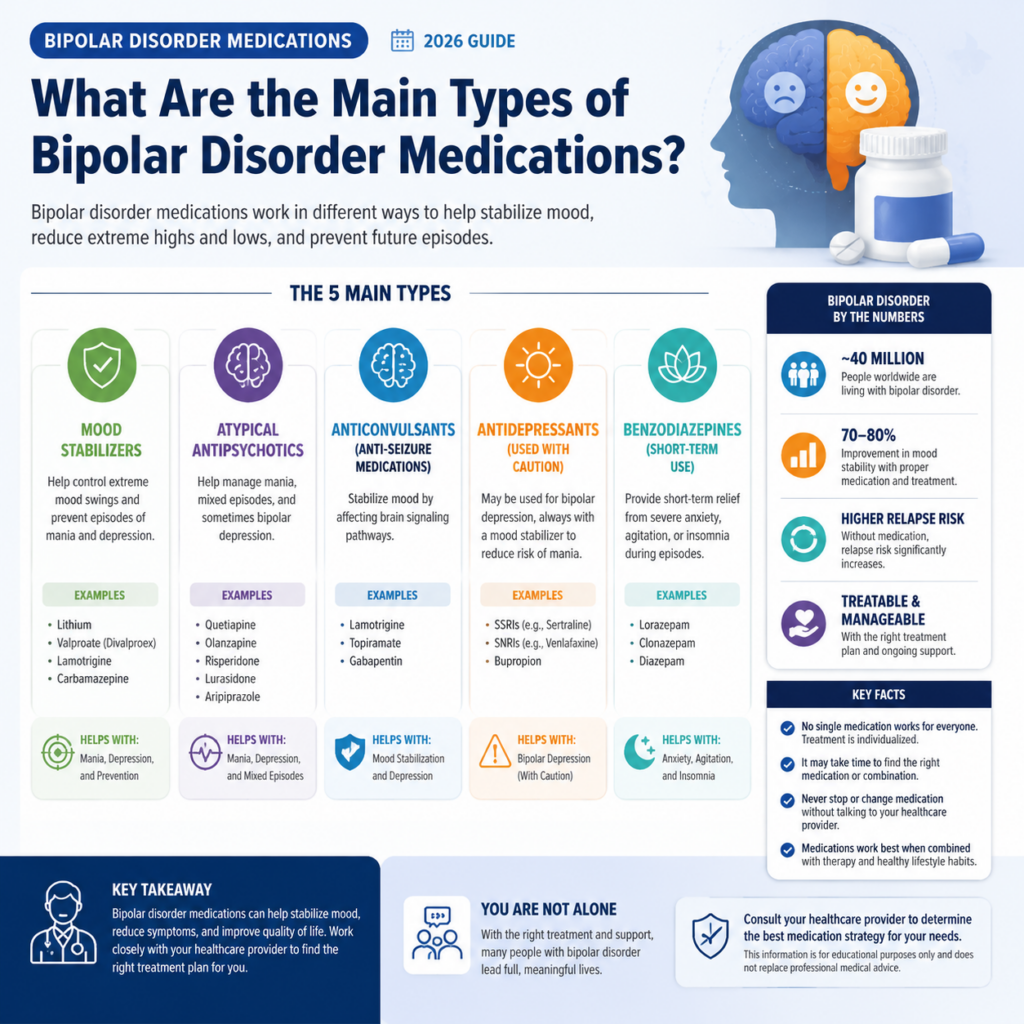
What Are the Main Types of Bipolar Disorder Medications?
Three primary medication classes treat bipolar disorder: mood stabilizers, atypical antipsychotics, and antidepressants, each targeting different aspects of the condition. Mood stabilizers prevent future episodes, antipsychotics address acute symptoms during manic or depressive phases, and antidepressants support recovery from depression when combined with stabilizers.
Mood Stabilizers: The Foundation
Mood stabilizers form the backbone of long-term bipolar treatment. These medications—lithium, valproate, carbamazepine, and lamotrigine—work by evening out the extreme highs and lows that define the disorder.
Lithium stands out as the most studied and effective option for bipolar I disorder. In my years following treatment research, I’ve watched lithium consistently outperform alternatives.
The numbers tell the story: people taking lithium stay relapse-free for a median of 81 months, while those on valproate manage only 36 months and carbamazepine 42 months. That’s more than double the stability.
Here’s what makes each mood stabilizer distinct:
Lithium: Best for classic bipolar I with clear manic episodes; requires regular blood tests to monitor kidney and thyroid function
Valproate (Depakote): Works well for mixed episodes and rapid cycling; causes less tremor than lithium but carries liver toxicity risk
Carbamazepine (Tegretol): Alternative when lithium fails; interacts with many medications through enzyme effects
Lamotrigine (Lamictal): Particularly effective for bipolar depression and bipolar II; low mania risk but requires slow dose titration to prevent rash
The choice between these depends on your specific pattern. If you experience rapid cycling—four or more episodes per year—valproate or carbamazepine might serve you better than lithium.
For bipolar II with predominant depression, lamotrigine often becomes the first choice.
Atypical Antipsychotics: Fast-Acting Relief
Atypical antipsychotics entered bipolar treatment in the 1990s and changed everything. Unlike older antipsychotics that mainly sedated patients, these newer medications actively reduce symptoms of both mania and depression.
Quetiapine (Seroquel) demonstrates particular strength in treating bipolar depression. Studies show it reduces depression scores significantly within eight weeks at doses of 300-600 mg daily, with improvements visible as early as week one. Both bipolar I and II patients respond similarly.
Olanzapine (Zyprexa) excels during acute mania. About 70% of people with bipolar I mania achieve symptomatic remission on olanzapine, with half reaching that point within eight weeks.
More importantly, 35% maintain sustained recovery over approximately 28 weeks—meaning they’re not just symptom-free but functioning well in daily life.
Other effective options include:
Risperidone (Risperdal): Strong anti-manic effects; higher risk of movement side effects
Aripiprazole (Abilify): Lower weight gain profile; works for both acute mania and maintenance
Lurasidone (Latuda): FDA-approved specifically for bipolar depression; must be taken with food
Cariprazine (Vraylar): Newer option for mania and depression; long half-life allows once-daily dosing
Bysanti (milsaperidone), approved by the FDA in early 2026, joins this group as a treatment for acute manic and mixed episodes in bipolar I disorder. It’s bioequivalent to iloperidone and brings over 100,000 patient-years of safety data, with U.S. availability expected later this year.
The main drawback? Weight gain and metabolic changes affect many people on these medications.
Olanzapine and quetiapine carry the highest risk, while aripiprazole and lurasidone cause less weight gain. You’ll need regular monitoring of weight, blood sugar, and cholesterol.
Antidepressants: Use With Caution
Antidepressants work differently in bipolar disorder than in regular depression. They help, but they also carry risks that don’t exist in unipolar depression.
When combined with mood stabilizers, antidepressants like SSRIs (fluoxetine, sertraline) and SNRIs (venlafaxine, duloxetine) produce response rates of 40-60% in bipolar depression. That’s moderate success—not spectacular, but meaningful for many people. Bipolar II patients tend to respond better than those with bipolar I.
The catch: up to 25% of people taking antidepressants without adequate mood stabilization experience a switch into mania or hypomania. This risk climbs higher with tricyclic antidepressants and drops somewhat with SSRIs. Some people also develop rapid cycling—more frequent mood episodes—when taking antidepressants long-term.
Common mistake: Starting an antidepressant without a mood stabilizer already on board. Always establish mood stabilization first, then add the antidepressant if depression persists.
And if you notice increased energy, decreased sleep need, or racing thoughts after starting an antidepressant, contact your doctor immediately—these signal a potential manic switch.

How Do Bipolar Disorder Medications Work for Different Subtypes?
Medication effectiveness varies significantly between bipolar I, bipolar II, and rapid-cycling presentations. Bipolar I responds best to lithium and antipsychotics for mania prevention, bipolar II often requires lamotrigine or antidepressant combinations for predominant depression, and rapid cycling may need valproate or carbamazepine due to their broader mood-stabilizing effects across episode types.
Bipolar I: Preventing Mania
If you have bipolar I disorder—characterized by full manic episodes lasting at least seven days—your primary treatment goal centers on preventing those manic episodes while also addressing depression. Mania causes the most damage: hospitalization, risky behavior, broken relationships, lost jobs.
Lithium excels here. In head-to-head comparisons, lithium reduces rehospitalization rates to 26% over 2.5 years compared to 62% with carbamazepine. That’s a massive difference when you consider what hospitalization means for your life, work, and family.
For acute mania—when you’re in the middle of an episode—atypical antipsychotics work faster than mood stabilizers. Olanzapine, risperidone, and quetiapine can reduce manic symptoms within days, while lithium takes 1-2 weeks to reach therapeutic levels. Many doctors prescribe both: an antipsychotic for immediate relief and lithium for long-term prevention.
Choose lithium if: You have classic bipolar I with clear manic episodes, no kidney disease, and can commit to regular blood monitoring.
Choose valproate if: You have mixed episodes (mania and depression simultaneously), rapid cycling, or can’t tolerate lithium’s side effects.
Add an antipsychotic if: You’re currently manic, have psychotic symptoms, or haven’t responded adequately to mood stabilizers alone.
Bipolar II: Targeting Depression
Bipolar II looks different. You experience hypomania—elevated mood that doesn’t quite reach full mania—but your main struggle comes from depression. The depressive episodes last longer, occur more frequently, and cause more functional impairment than the hypomanic periods.
Lamotrigine becomes the star player for bipolar II. It prevents depressive episodes without triggering hypomania, a rare quality among bipolar medications. Studies show 56% of people taking 200 mg daily achieve greater than 50% improvement in depression scores, compared to 29% on placebo.
The downside?
It takes 6-8 weeks to reach therapeutic doses due to rash risk with faster titration.
Quetiapine also works well for bipolar II depression, with similar effectiveness to bipolar I. The advantage: faster onset than lamotrigine. The disadvantage: more sedation and weight gain.
Antidepressants play a bigger role in bipolar II than bipolar I, but you still need a mood stabilizer foundation. The switch risk exists but runs lower than in bipolar I. Many people with bipolar II do well on lamotrigine plus an SSRI, a combination that addresses both mood stability and depression.
I’ve noticed that bipolar II often gets undertreated because hypomania doesn’t seem as serious as mania. But the depression hits just as hard, and the suicide risk runs just as high.
Don’t let the “II” fool you into thinking it’s milder—it’s different, requiring different medication strategies.
For more on distinguishing these subtypes, read what is the difference between bipolar I and bipolar II.
Rapid Cycling: The Toughest Challenge
Rapid cycling means four or more mood episodes per year. It’s harder to treat, responds less predictably to medications, and often requires combination therapy from the start.
Lithium works less well in rapid cycling than in classic bipolar I. Valproate and carbamazepine show better results, possibly because they stabilize mood through different mechanisms—affecting sodium channels and GABA systems rather than lithium’s effects on intracellular signaling.
Combination therapy becomes necessary for many people with rapid cycling. Studies of valproate plus lithium, or valproate plus carbamazepine, show that combinations reduce the frequency of episodes more than either medication alone. The trade-off: more side effects and more complex monitoring.
One pattern I’ve seen repeatedly: rapid cycling often develops after years of antidepressant use without adequate mood stabilization. If you’re cycling rapidly, review your medication history with your doctor. Stopping the antidepressant and optimizing mood stabilizers might slow the cycling.
Edge case: Some people develop rapid cycling due to thyroid problems, even subclinical hypothyroidism that wouldn’t cause symptoms in someone without bipolar disorder.
If you’re rapid cycling despite good medication adherence, ask your doctor to check your thyroid function carefully, including TSH, free T4, and thyroid antibodies.
What Are the Most Common Side Effects of Bipolar Disorder Medications?
Side effects vary by medication class but commonly include weight gain, sedation, tremor, and metabolic changes with antipsychotics; kidney and thyroid effects with lithium; liver toxicity and hair loss with valproate; and rash with lamotrigine.
Most side effects are manageable through dose adjustment, medication switching, or supportive treatments, but some require regular monitoring to prevent serious complications.
Mood Stabilizer Side Effects
Lithium requires the most monitoring but remains remarkably safe when managed properly. The main concerns:
Kidney effects: Long-term lithium can reduce kidney function, though severe damage is rare with proper monitoring. You’ll need blood tests for kidney function every 6-12 months.
Thyroid problems: About 20% of people on lithium develop hypothyroidism, easily treated with thyroid hormone replacement. Annual thyroid checks catch this early.
Tremor: Fine hand tremor affects many people, sometimes improving with dose reduction or beta-blocker addition.
Weight gain: Moderate, averaging 10-15 pounds, less than most antipsychotics.
Thirst and urination: Increased fluid intake and urination are common but usually tolerable.
The therapeutic window for lithium is narrow—the difference between an effective dose and a toxic dose is small. That’s why blood level monitoring every 3-6 months is essential. Dehydration, NSAIDs like ibuprofen, and some blood pressure medications can push lithium levels into the toxic range.
Valproate causes different problems:
Weight gain: Often more than lithium, averaging 15-20 pounds
Hair loss: Temporary thinning in some people; zinc and selenium supplements may help
Tremor: Similar to lithium
Liver toxicity: Rare but serious; requires liver function tests at baseline and periodically
Polycystic ovary syndrome: Risk in women of childbearing age
Birth defects: High risk during pregnancy; not recommended for women planning pregnancy
Carbamazepine brings its own set of concerns:
Drug interactions: Extensive, because it speeds up metabolism of many medications including birth control pills
Blood cell effects: Rare risk of low white blood cells; requires blood count monitoring
Rash: Occurs in about 10% of people, usually mild but occasionally serious
Dizziness and coordination problems: Especially when starting or increasing dose
Lamotrigine has the best tolerability profile among mood stabilizers:
Rash: The main concern, occurring in 10% of people. Serious rash (Stevens-Johnson syndrome) is rare (0.1%) but requires immediate medical attention. Slow dose titration reduces risk.
Headache: Common initially, usually improves
Minimal weight gain: One of the few bipolar medications that doesn’t typically cause weight gain
No sedation: Unlike most other options
For detailed information on managing these effects, visit our page on common side effects of bipolar disorder medications.
Antipsychotic Side Effects
Atypical antipsychotics share several common side effects, though severity varies by specific medication:
Metabolic effects top the list:
Weight gain: Ranges from 10-30 pounds on average, highest with olanzapine and clozapine, lowest with aripiprazole and lurasidone
Diabetes risk: Increased blood sugar and insulin resistance, sometimes leading to type 2 diabetes
Cholesterol elevation: Particularly triglycerides
Metabolic syndrome: The combination of weight gain, high blood sugar, high cholesterol, and high blood pressure
Sedation affects many people, especially with quetiapine and olanzapine. Taking the medication at bedtime helps, and tolerance often develops over weeks. But some people remain too sedated for normal functioning, requiring a medication switch.
Movement effects occur less with atypical antipsychotics than older ones but still happen:
Akathisia: Inner restlessness, feeling like you can’t sit still
Tremor: Similar to lithium tremor
Tardive dyskinesia: Involuntary movements, usually of the face and tongue; risk increases with years of use
Prolactin elevation with risperidone and paliperidone can cause:
Breast enlargement and milk production in both men and women
Menstrual irregularities
Sexual dysfunction
Bone density loss with long-term elevation
Quetiapine specifically causes dry mouth, constipation, and dizziness in many people. Despite these effects, 59% of people in studies completed the full treatment course, suggesting tolerability is acceptable for most.
Antidepressant Side Effects in Bipolar Disorder
Beyond the standard antidepressant side effects—nausea, sexual dysfunction, sleep changes—bipolar disorder adds unique risks:
Mania induction: Up to 25% risk without adequate mood stabilization
Rapid cycling: Increased episode frequency with long-term use
Mixed states: Simultaneous depression and activation, often more distressing than either alone
Standard SSRI side effects include:
Sexual dysfunction (decreased libido, delayed orgasm, erectile problems)
Weight gain (usually 5-15 pounds)
Gastrointestinal upset initially
Sleep changes (insomnia with some, sedation with others)
Decision rule: If you develop increased energy, decreased sleep need, racing thoughts, or increased goal-directed activity within weeks of starting an antidepressant, contact your doctor immediately. These signal a potential switch into hypomania or mania, requiring prompt intervention.
What New Bipolar Disorder Medications Are Available in 2026?
Several promising medications entered clinical use or advanced trials in 2026, including Bysanti for acute mania, AL001 lithium delivery system in Phase 2 trials, BXCL501 for at-home agitation treatment nearing approval, and endoxifen in Phase 3 testing for bipolar I mania.
These innovations address unmet needs like reduced toxicity, at-home crisis management, and novel mechanisms beyond traditional mood stabilizers.
Bysanti: New FDA-Approved Option
The FDA approved Bysanti (milsaperidone) in early 2026 for acute manic and mixed episodes in bipolar I disorder. Developed by Vanda Pharmaceuticals, it’s bioequivalent to iloperidone, an existing antipsychotic, but brings over 100,000 patient-years of safety data to support its use.
What makes Bysanti notable isn’t a revolutionary mechanism—it works like other atypical antipsychotics through dopamine and serotonin receptor effects—but rather its established safety profile and availability as another option when other antipsychotics cause intolerable side effects. U.S. availability is expected later in 2026.
AL001: Safer Lithium Delivery
AL001, developed by Alzamend Neuro, entered Phase 2 clinical trials in early 2026. This novel lithium delivery system aims to provide lithium’s therapeutic benefits while minimizing toxicity risks like kidney damage and thyroid dysfunction.
The concept addresses lithium’s biggest limitation: its narrow therapeutic window and long-term organ effects. If successful, AL001 could make lithium accessible to people who currently can’t take it due to kidney disease or who discontinue it due to side effects. Results from the Phase 2 trial should emerge in 2027.
This development matters because lithium remains the most effective medication for bipolar I disorder, yet many people can’t take it or stop it due to side effects. A safer formulation could help more people benefit from lithium’s superior relapse prevention.
BXCL501: At-Home Agitation Treatment
BXCL501 (dexmedetomidine) completed database lock in a pivotal Phase 3 trial in 2026, evaluating at-home treatment of agitation in bipolar I and II disorders. The SERENITY At-Home trial enrolled over 200 patients, and the FDA granted Fast Track designation.
Currently marketed as Igalmi for inpatient use, BXCL501 could become the first FDA-approved at-home treatment for agitation in bipolar disorders if approved for outpatient use. This would represent a significant advance, allowing people to manage agitation episodes at home rather than requiring emergency room visits or hospitalization.
The medication works through alpha-2 adrenergic receptors, calming agitation without the heavy sedation of typical antipsychotics. It’s administered as a sublingual film, making it practical for home use during crisis situations.
Endoxifen: Novel Mechanism
Endoxifen, derived from the breast cancer drug tamoxifen, is in Phase 3 trials for acute manic episodes in bipolar I disorder. It works through estrogen pathways, a completely different mechanism from traditional mood stabilizers or antipsychotics.
Prior studies showed 8 mg doses reduced Young Mania Rating Scale scores and decreased the need for additional medications. Endoxifen is already approved in India specifically for bipolar I disorder, providing real-world evidence of its effectiveness.
This novel mechanism matters because about one-third of people with bipolar disorder don’t respond adequately to current medications. New mechanisms offer hope for these treatment-resistant cases.
COMP360: Psilocybin for Bipolar Depression
COMP360, COMPASS Pathways’ synthetic psilocybin, entered Phase 3 trials in early 2026 for treatment-resistant depression. While not specifically designed for bipolar disorder, early data suggests potential for bipolar depression without inducing mania, drawing significant clinician interest.
Psilocybin works through serotonin 2A receptor agonism, producing rapid antidepressant effects that can last weeks or months after a single dose. The bipolar application remains experimental, but the possibility of rapid, sustained depression relief without mania risk would fill a major treatment gap.
Caution: Psilocybin remains investigational for bipolar disorder. Don’t attempt self-medication with recreational psilocybin, which lacks dosing control, medical supervision, and the therapeutic framework used in clinical trials.
Research Insights: Lithium and Metformin
Beyond new medications, 2026 research published in The Lancet elucidated how lithium works through AMPK pathways in the brain. This discovery points toward next-generation therapies, including metformin—already FDA-approved for diabetes and used by millions—as a potential treatment for people who don’t respond to lithium.
The research matters because people with bipolar disorder face twice the risk of type 2 diabetes and 50% show insulin resistance. Metformin addresses both the metabolic complications of bipolar medications and potentially the mood symptoms themselves through AMPK activation.
Several medical centers are now studying metformin as an adjunctive treatment in bipolar disorder, particularly for people with metabolic syndrome or those who haven’t responded to standard mood stabilizers.
For more on treatment approaches, see our guide on dealing with bipolar disorder.
How Should You Work With Your Doctor on Bipolar Disorder Medications?
Effective medication management requires active partnership with your psychiatrist, including honest reporting of symptoms and side effects, regular monitoring through blood tests and appointments, patience during the 6-12 week trial period needed to assess medication effectiveness, and collaborative decision-making about dose adjustments or medication changes.
Keep a mood chart tracking sleep, energy, and mood daily to provide objective data for treatment decisions.
Start With Accurate Diagnosis
Medication selection depends entirely on accurate diagnosis. Bipolar disorder gets misdiagnosed as unipolar depression in about 40% of cases initially, leading to antidepressant monotherapy that can worsen outcomes.
Before starting medication, make sure your doctor has:
Complete episode history: When did mood episodes start? How long did they last? What were the symptoms?
Family history: Bipolar disorder runs in families; family history helps confirm diagnosis
Substance use assessment: Stimulants, alcohol, and other substances can mimic or trigger mood episodes
Medical workup: Thyroid problems, neurological conditions, and other medical issues can cause mood symptoms
If you’ve never had a manic or hypomanic episode, you don’t have bipolar disorder—you have unipolar depression, which requires different treatment. Conversely, if you’ve had clear manic episodes but were diagnosed with depression, you need bipolar-specific treatment.
For more on getting the right diagnosis, visit our page on bipolar disorder diagnosis.
Set Realistic Expectations
Medications work, but they’re not magic. Here’s what to expect:
Timeline for improvement:
Acute mania: 1-2 weeks for noticeable improvement with antipsychotics
Acute depression: 2-4 weeks for initial response, 6-8 weeks for full effect
Maintenance/prevention: 3-6 months to assess whether relapses are prevented
Degree of improvement:
Complete symptom elimination: Uncommon
Significant reduction allowing normal functioning: Realistic goal for most people
Residual symptoms requiring additional strategies: Common, especially mild depression
Medication trials:
First medication works adequately: About 50% of people
Need to try 2-3 medications to find the right one: About 40% of people
Require combination therapy: About 30% of people
Treatment-resistant requiring multiple combinations: About 10-15% of people
I’ve watched too many people give up on medication after one failed trial. Finding the right medication often takes persistence. The first medication might not work, but the third one might change your life.
Track Your Response
Objective data helps you and your doctor make better decisions. Keep a daily mood chart tracking:
Sleep: Hours slept, sleep quality, difficulty falling asleep or staying asleep
Energy: Rated 1-10, with 5 being normal
Mood: Rated 1-10, with 5 being neutral, 1 being severely depressed, 10 being manic
Irritability: Rated 1-10
Anxiety: Rated 1-10
Medications: Doses taken, any missed doses
Side effects: Any new or worsening side effects
Life events: Stressors, conflicts, positive events
Several apps make this easier, including Daylio, eMoods, and Mood Tracker. Or use a simple spreadsheet or paper chart. The format matters less than consistency.
Bring your mood chart to appointments. It provides objective data about patterns you might not remember or recognize. I’ve seen mood charts reveal patterns that changed treatment decisions—like depression worsening every time an antidepressant dose increased, or hypomania appearing three days after sleep disruption.
Communicate About Side Effects
Don’t suffer in silence. Most side effects can be managed through:
Dose adjustment: Lower doses often reduce side effects while maintaining effectiveness
Timing changes: Taking sedating medications at bedtime, activating ones in the morning
Supportive treatments: Metformin for weight gain, propranolol for tremor, etc.
Medication switching: If side effects remain intolerable despite adjustments
Common mistake: Stopping medication abruptly due to side effects without consulting your doctor. This can trigger rebound mood episodes. Always discuss side effects before making changes.
Be specific when reporting side effects. Instead of “I feel terrible,” say “I’ve gained 12 pounds in six weeks, I’m sleeping 10 hours a night and still feel tired, and I can’t concentrate at work.” Specific information allows specific solutions.
Understand Monitoring Requirements
Different medications require different monitoring:
Lithium:
Blood level: Every 3-6 months once stable, more often when adjusting dose
Kidney function: Every 6-12 months
Thyroid function: Annually
Calcium: Annually
Valproate:
Blood level: Every 3-6 months once stable
Liver function: Baseline, then periodically
Blood counts: Baseline, then periodically
Pregnancy test: Before starting in women of childbearing age
Carbamazepine:
Blood level: Every 3-6 months once stable
Blood counts: Baseline, then every 3-6 months
Liver function: Baseline, then periodically
Antipsychotics:
Weight: Every visit
Blood pressure: Every visit
Fasting glucose: Baseline, 3 months, then annually
Lipid panel: Baseline, 3 months, then annually
Movement assessment: Every visit
Lamotrigine:
No routine blood monitoring required
Watch for rash, especially in first 8 weeks
Missing monitoring appointments can lead to serious complications going undetected. If you’re having trouble keeping up with appointments, talk to your doctor about simplifying the schedule or using home monitoring for some parameters.
For more on working effectively with healthcare providers, read our guide on working with your doctor.

What Happens When First-Line Medications Don’t Work?
About one-third of people with bipolar disorder don’t respond adequately to initial medication trials, requiring combination therapy, higher doses, medication switches, or augmentation strategies.
Treatment-resistant bipolar disorder benefits from systematic approaches including ensuring adequate medication trials (correct dose for sufficient duration), addressing comorbid conditions like anxiety or substance use, and adding adjunctive treatments like thyroid hormone or omega-3 fatty acids.
Doctors also consider specialized interventions like electroconvulsive therapy for severe cases.
Ensure Adequate Trials First
Before declaring a medication ineffective, make sure you’ve given it a fair trial:
Adequate dose: Many people receive subtherapeutic doses due to side effect concerns. For example, lithium blood levels should reach 0.6-1.0 mEq/L for maintenance, higher for acute mania. Lamotrigine requires 200 mg daily for most people.
Sufficient duration: Mood stabilizers need 6-12 weeks at therapeutic doses to show full preventive effects. Stopping at 4 weeks might miss the benefit.
Good adherence: Missing doses regularly undermines effectiveness. If you’re missing doses due to side effects or complexity, address those issues before concluding the medication doesn’t work.
Appropriate target: If you’re taking lithium for bipolar depression, it might not help much—lithium works better for mania prevention. Matching medication to your specific symptoms matters.
Combination Strategies
When monotherapy fails, combinations often succeed. Studies show:
Lithium plus valproate: Reduces recurrence frequency more than either alone, though mixed episodes may increase
Mood stabilizer plus antipsychotic: Standard for many people, combining prevention with acute symptom control
Valproate plus carbamazepine: Yields moderate to marked responses in 100% of previously refractory manic patients in some studies
The challenge with combinations: more side effects, more complex monitoring, higher costs, and increased risk of drug interactions. But for people who don’t respond to monotherapy, combinations can mean the difference between constant cycling and stability.
Choose combinations when:
You’ve tried at least two monotherapy options at adequate doses and durations
You have partial response to monotherapy but need additional improvement
You have mixed episodes or rapid cycling that typically require combination therapy
You have severe symptoms requiring faster or more complete control
Augmentation Approaches
Augmentation means adding a medication that isn’t typically used alone for bipolar disorder but enhances the effect of your primary medication:
Thyroid hormone: Even people with normal thyroid function sometimes benefit from T3 (liothyronine) or T4 (levothyroxine) augmentation, particularly for depression and rapid cycling.
Omega-3 fatty acids: EPA (eicosapentaenoic acid) at doses of 1-2 grams daily shows modest antidepressant effects in some studies with minimal side effects.
N-acetylcysteine (NAC): An antioxidant that may reduce depressive symptoms; doses of 2 grams daily used in studies.
Metformin: Beyond treating metabolic side effects, emerging evidence suggests mood benefits through AMPK pathway effects.
Stimulants: Controversial but sometimes used for persistent depression or ADHD comorbidity; requires careful monitoring for mania induction.
These augmentation strategies typically add modest benefits—not dramatic transformations—but modest improvement can be meaningful when you’re struggling despite standard treatments.
When to Consider ECT
Electroconvulsive therapy (ECT) remains the most effective treatment for severe bipolar depression and mixed episodes, with response rates of 70-80% even in treatment-resistant cases. Modern ECT uses anesthesia and muscle relaxants, making it safe and well-tolerated.
Consider ECT when:
You’ve failed multiple medication trials
You’re severely depressed with suicidal thoughts
You can’t tolerate medications due to side effects or medical conditions
You need rapid response due to severity (catatonia, psychosis, severe suicidality)
You’ve responded well to ECT in the past
The main drawback: memory effects, particularly for events around the treatment period. Most memory issues resolve within weeks to months, though some people report persistent gaps.
ECT isn’t a last resort—it’s an effective treatment option that should be considered when medications aren’t working adequately. The stigma around ECT has decreased as techniques have improved and safety has been established.
For additional support strategies beyond medication, explore our bipolar disorder support resources.
How Do Lifestyle Factors Affect Bipolar Disorder Medications?
Sleep, exercise, diet, substance use, and stress management significantly impact medication effectiveness and mood stability. Irregular sleep can trigger episodes even with optimal medication, alcohol and drugs interact dangerously with bipolar medications and destabilize mood.
Research proves that regular exercise enhances medication response and reduces depression, and consistent daily routines support the circadian rhythm regulation that medications work to establish.
Sleep: The Foundation
Sleep disruption triggers mood episodes more reliably than almost any other factor. Missing even one night of sleep can precipitate mania in vulnerable individuals, while oversleeping often signals emerging depression.
Sleep hygiene essentials:
Same bedtime and wake time every day, including weekends
7-9 hours of sleep nightly
Dark, cool, quiet bedroom
No screens for 1 hour before bed
No caffeine after 2 PM
No alcohol within 3 hours of bedtime
Many bipolar medications cause sedation, which can help with sleep but also lead to oversleeping. Set an alarm and get up at the same time daily, even if you feel tired. Consistent wake time regulates your circadian rhythm more effectively than consistent bedtime.
Warning sign: If you suddenly need less sleep but don’t feel tired, contact your doctor immediately. This often signals emerging mania, requiring prompt intervention before it escalates.
Substance Use: A Dangerous Combination
Alcohol and drugs don’t mix with bipolar disorder or its medications. About 50% of people with bipolar disorder develop substance use problems at some point, often starting as self-medication attempts.
Alcohol:
Interacts with mood stabilizers, increasing sedation and side effects
Disrupts sleep architecture, triggering mood episodes
Worsens depression directly through its depressant effects
Impairs judgment about medication adherence
Cannabis:
May trigger psychosis or mania in vulnerable individuals
Worsens motivation and cognition, particularly with regular use
Interacts with some medications through liver enzyme effects
Stimulants (cocaine, methamphetamine, prescription stimulants):
Directly trigger mania or mixed episodes
Interfere with sleep, compounding risk
Can cause psychosis indistinguishable from bipolar psychosis
Nicotine:
Doesn’t directly trigger mood episodes but affects medication metabolism
Smoking increases metabolism of some medications, requiring higher doses
Quitting can increase medication blood levels, requiring dose adjustment
For more on this topic, read how does nicotine affect your bipolar disorder.
If you’re struggling with substance use, address it as part of your treatment plan. Integrated treatment for both bipolar disorder and substance use works better than treating them separately. For resources, visit our page on navigating the dual challenges of bipolar disorder and substance abuse.
Exercise: Natural Mood Stabilization
Regular exercise enhances medication effectiveness and provides independent mood benefits. Studies show exercise reduces depressive symptoms, improves sleep, decreases anxiety, and may help prevent manic episodes through stress reduction.
Effective exercise for bipolar disorder:
Moderate intensity: 30-45 minutes most days
Consistency matters more than intensity: Daily walks beat occasional intense workouts
Morning or afternoon timing: Evening exercise can interfere with sleep
Variety helps adherence: Mix cardio, strength training, yoga, outdoor activities
Caution during mania: Excessive exercise can be a symptom of mania rather than healthy behavior. If you’re suddenly exercising for hours daily with little rest, this may signal an episode rather than wellness.
Diet and Metabolism
Bipolar medications, particularly antipsychotics and valproate, often cause weight gain and metabolic changes. Proactive dietary strategies help:
Preventive nutrition:
Mediterranean-style diet: Emphasize vegetables, fruits, whole grains, fish, olive oil
Limit processed foods and added sugars
Regular meal timing to support circadian rhythms
Adequate protein to support satiety and stable blood sugar
Omega-3 fatty acids: Found in fatty fish (salmon, mackerel, sardines) or supplements; may provide modest mood benefits beyond cardiovascular health.
Avoid crash diets: Severe calorie restriction can trigger mood episodes. If you need to lose weight gained from medications, aim for gradual loss of 1-2 pounds weekly through moderate calorie reduction and increased activity.
Some people find that certain foods affect their mood, though evidence is limited. If you notice patterns—like sugar crashes triggering depression or caffeine worsening anxiety—adjust accordingly. But don’t eliminate entire food groups without medical guidance.
For more on lifestyle approaches, see our guide on lifestyle changes for bipolar disorder.
Stress Management
Stress triggers mood episodes even with optimal medication. Effective stress management isn’t optional—it’s essential for stability.
Evidence-based stress reduction:
Mindfulness meditation: 10-20 minutes daily reduces stress reactivity
Cognitive-behavioral therapy: Helps identify and modify stress-generating thought patterns
Social rhythm therapy: Maintains regular daily routines to buffer against stress
Boundaries: Learning to say no, limiting commitments, protecting sleep and self-care time
Early warning signs: Develop a list of your personal early warning signs for both mania and depression. Common signs include sleep changes, irritability, social withdrawal, increased goal-directed activity, or racing thoughts. When you notice these, implement your crisis plan: contact your doctor, increase monitoring, reduce stress, ensure medication adherence.
For structured approaches, read about interpersonal and social rhythm therapy and psychoeducation and early intervention.
Frequently Asked Questions About Bipolar Disorder Medications
How long do I need to take bipolar disorder medications?
Most people with bipolar disorder need long-term medication, often lifelong, because the condition is chronic and relapse risk remains high after stopping medication. Studies show 90% of people who stop mood stabilizers experience relapse within 5 years, compared to 40% who continue treatment. After a single manic episode, some doctors recommend at least 2 years of treatment before considering discontinuation, but most experts advise indefinite treatment after multiple episodes.
Can I stop taking medication if I feel better?
Feeling better usually means the medication is working, not that you no longer need it. Stopping medication when stable is the most common cause of relapse. If you want to try reducing or stopping medication, work with your doctor to taper gradually while monitoring closely for early warning signs. Never stop abruptly, as this can trigger severe rebound episodes.
What should I do if I miss a dose?
Take the missed dose as soon as you remember, unless it’s close to your next scheduled dose. Don’t double up doses. If you miss multiple doses, contact your doctor before resuming, as some medications require retitration. Missing doses occasionally usually doesn’t cause immediate problems, but patterns of missed doses significantly increase relapse risk.
Are bipolar disorder medications safe during pregnancy?
Medication safety during pregnancy varies by drug. Valproate carries high risk of birth defects and should be avoided. Lithium carries moderate risk, particularly of heart defects. Lamotrigine appears relatively safer. Antipsychotics vary, with quetiapine and lurasidone having more safety data. The risk of untreated bipolar disorder during pregnancy—including postpartum psychosis—must be weighed against medication risks. Work with a psychiatrist experienced in perinatal mental health to develop a plan before pregnancy if possible. For more information, read how does pregnancy affect someone with bipolar disorder.
Will medications change my personality?
Effective bipolar medications should stabilize your mood without fundamentally changing your personality. You should still feel like yourself, just without the extreme mood swings. If you feel emotionally numb, flat, or unlike yourself, discuss this with your doctor—it may indicate overmedication or the wrong medication. Some people worry that treating hypomania will eliminate their creativity or energy, but most find they’re more consistently productive when stable than when cycling.
How do I know if my medication is working?
Medication effectiveness shows up in several ways: fewer mood episodes, less severe episodes when they occur, faster recovery from episodes, better functioning between episodes, and improved quality of life. Track your mood, sleep, and functioning over months, not days. Some improvement should be visible within 4-8 weeks for acute treatment, but full preventive effects take 3-6 months to assess.
What if I can’t afford my medications?
Medication costs create real barriers. Options include: asking your doctor about generic alternatives (available for lithium, valproate, carbamazepine, lamotrigine, and some antipsychotics), applying for pharmaceutical company patient assistance programs, checking if you qualify for Medicaid or Medicare, using prescription discount cards like GoodRx, and asking your pharmacist about lower-cost options. Never skip doses to make medication last longer—this increases relapse risk and often leads to more expensive hospitalizations.
Can I drink alcohol while taking bipolar medications?
Alcohol is generally not recommended with bipolar medications. It increases sedation and side effects, disrupts sleep and mood stability, interferes with medication effectiveness, and impairs judgment about medication adherence. Occasional light drinking (1-2 drinks) may be tolerated by some people on some medications, but discuss this with your doctor. Heavy drinking or binge drinking is particularly dangerous, both for medication interactions and for triggering mood episodes.
Do bipolar disorder medications cause weight gain?
Many bipolar medications cause weight gain, but the amount varies significantly. Highest risk: olanzapine, clozapine, valproate. Moderate risk: quetiapine, risperidone, lithium. Lower risk: lamotrigine, aripiprazole, lurasidone, ziprasidone. Weight gain typically occurs in the first 6 months of treatment. Proactive strategies—monitoring weight weekly, adjusting diet, increasing exercise, considering metformin—can limit gain. If you gain more than 10% of body weight, discuss medication adjustment with your doctor.
Can I take supplements with bipolar medications?
Some supplements interact with bipolar medications or affect mood. Always tell your doctor about supplements you’re taking. Potentially helpful: omega-3 fatty acids, vitamin D (if deficient), folate. Use with caution: St. John’s wort (interacts with many medications and may trigger mania), SAMe (may trigger mania), high-dose B vitamins (may interfere with mood stabilizers). Generally safe: multivitamin, calcium, vitamin D at recommended doses.
What happens if I need surgery while taking bipolar medications?
Most bipolar medications can be continued through surgery, but inform your surgeon and anesthesiologist about all medications. Lithium may need to be held 24-48 hours before major surgery due to interaction with anesthesia and fluid shifts. MAOIs (rarely used for bipolar disorder) require special anesthetic considerations. Don’t stop mood stabilizers without medical guidance, as this increases risk of postoperative mood episodes.
How do I manage side effects that won’t go away?
Persistent side effects require a systematic approach: ensure you’re taking the lowest effective dose, try timing adjustments (bedtime for sedating medications), add supportive treatments for specific side effects (metformin for weight gain, propranolol for tremor), consider switching to a medication with a different side effect profile, or accept tolerable side effects if the medication is highly effective. The goal is finding the best balance between effectiveness and tolerability for your individual situation.
Taking Control of Your Treatment Journey
Medications form the foundation of effective bipolar disorder treatment, but finding the right regimen takes time, patience, and active partnership with your healthcare team. Lithium remains the gold standard for bipolar I maintenance, extending relapse-free periods to 81 months on average.
Atypical antipsychotics like quetiapine provide rapid relief for both manic and depressive episodes. Lamotrigine excels for bipolar II and depression prevention. And new 2026 options—including Bysanti, AL001, and BXCL501—offer additional tools for people who haven’t found success with existing treatments.
The path to stability rarely follows a straight line. You might need to try several medications before finding the right one. You’ll probably need to adjust doses, manage side effects, and possibly combine medications.
About one-third of people need combination therapy to achieve adequate control. But persistence pays off—most people with bipolar disorder eventually find a medication regimen that allows them to live full, productive lives.
Your next steps:
Track your symptoms daily using a mood chart or app to provide objective data for treatment decisions
Schedule regular appointments with your psychiatrist, even when you’re feeling stable
Get required monitoring blood tests and health checks to catch problems early
Build your support system including therapy, support groups, and trusted friends or family
Maintain healthy routines for sleep, exercise, and stress management to support medication effectiveness
Educate yourself about bipolar disorder, treatment options, and self-management strategies
Develop a crisis plan with early warning signs and steps to take if you notice symptoms returning
Remember that medication is just one part of comprehensive bipolar disorder management. Therapy, lifestyle changes, social support, and self-monitoring all contribute to long-term stability. For additional resources and support, explore our bipolar disorder tools and mental health resources.
You didn’t choose to have bipolar disorder, but you can choose how you respond to it.
With the right medications, professional support, and personal commitment, you can achieve stability and build the life you want. The journey takes effort, but you don’t have to walk it alone.
Download tools that can help you remember to take your medication as prescribed.
- Medication List and Information Chart (PDF)
- Prescription Refill and Medical Testing Log (PDF)
- Psychotherapy can also help patients with bipolar disorder, and is often used in combination with medication. Learn more about talk therapy.